
Page 129 - Physiological based CPAP for preterm infants at birth Tessa Martherus
P. 129
Feasibility and effect of physiological based CPAP in preterm infants at birth
P
125
5
r
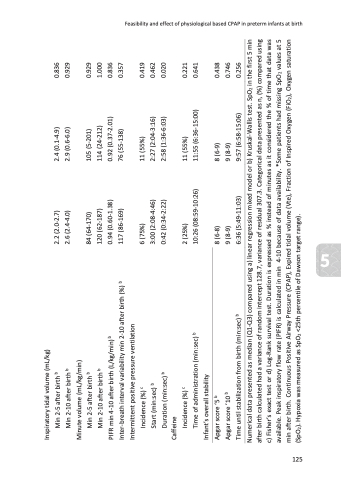
Inspiratory tidal volume (mL/kg) Min 2-5 after birth b
Min 2-10 after birth b
2.2 (2.0-2.7) 2.6 (2.4-4.0)
2.4 (0.1-4.9) 2.9 (0.6-6.0)
0.836 0.929
Minute volume (mL/kg/min) Min 2-5 after birth b Min 2-10 after birth b
84 (64-170)
120 (62-187) 0.94 (0.60-1.38) 117 (86-169)
105 (5-201)
114 (24-212) 0.92 (0.37-2.01) 76 (55-138)
0.929 1.000 0.836 0.357
PIFR min 4-10 after birth (L/kg/min) b
Inter-breath interval variability min 2-10 after birth (%) b Intermittent positive pressure ventilation
Incidence (%) c
Start (min:sec) b Duration (min:sec) b
6 (75%)
3:00 (2:08-4:46) 0:42 (0:34-2:22)
11 (55%)
2:27 (2:04-3:16) 2:58 (1:36-6:03)
0.419 0.462 0.020
Caffeine
Incidence (%) c
2 (25%)
10:26 (08:59-10:26)
11 (55%)
11:55 (6:36-15:00)
0.221 0.641
Time of administration (min:sec) b Infant’s overall stability
Apgar score ‘5 b
Apgar score ’10 b
8 (6-8)
9 (8-9)
6:36 (5:49-11:03)
8 (6-9)
9 (8-9)
9:57 (6:58-15:06)
0.438 0.746 0.256
Time until stabilization from birth (min:sec) b
Numerical data presented as median (Q1-Q3) compared using a) linear regression mixed model or b) Kruskal-Wallis test. SpO2 in the first 5 min after birth calculated had a variance of random intercept 128.7, variance of residual 307.3. Categorical data presented as n, (%) compared using c) Fisher’s exact test or d) Log-Rank survival test. Duration is expressed as % instead of minutes as it considered the % of time that data was available. Peak inspiratory flow rate (PIFR) is calculated in min 4-10 because of data availability. *Some patients had missing SpO2 values at 5 min after birth. Continuous Positive Airway Pressure (CPAP), Expired tidal volume (Vte), Fraction of Inspired Oxygen (FiO2), Oxygen saturation (SpO2). Hypoxia was measured as SpO2 <25th percentile of Dawson target range).
