
Page 46 - Strategies for non-invasive managementof high-grade cervical intraepithelial neoplasia - prognostic biomarkers and immunotherapy Margot Maria Koeneman
P. 46
Chapter 2
The profile was characterized by a sensitivity of 71%, specificity of 85%, PPV of 56% and NPV of 92%.
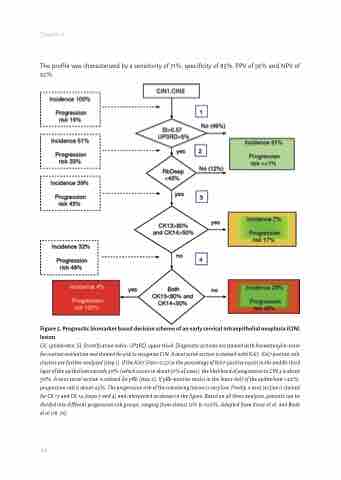
Figure 5. Prognostic biomarker‐based decision scheme of an early cervical intraepithelial neoplasia (CIN) lesion.
CK, cytokeratin; SI, Stratification Index; UP3RD, upper third. Diagnostic sections are stained with haematoxylin-eosin for routine evaluation and stained for p16 to recognize CIN. A next serial section is stained with Ki67. Ki67 positive cells clusters are further analysed (step 1). If the Ki67 SI90>0.57 or the percentage of Ki67-positive nuclei in the middle third layer of the epithelium exceeds 30% (which occurs in about 51% of cases), the likelihood of progression to CIN 3 is about 30%. A next serial section is stained for pRb (step 2). If pRb-positive nuclei in the lower half of the epithelium <40%, progression risk is about 43%. The progression risk of the remaining lesions is very low. Finally, a next section is stained for CK 13 and CK 14 (steps 3 and 4) and interpreted as shown in the figure. Based on all three analyses, patients can be divided into different progression risk groups, ranging from almost 0% to 100%. Adapted from Kruse et al. and Baak et al (18, 76)
44
